
2023: An English court convicts the parents of a 16-year-old girl of manslaughter for negligent care of their daughter, identifying as the primary cause of death letting her become fatally obese. The girl had in fact grown to weigh 146 kg and had a body mass index of 70 percent. [1]
2024: The first lawsuit is filed in Pennsylvania against large food companies, accusing them of creating harmful and addictive ultra-processed foods. The plaintiff, Bryce Martinez, was diagnosed with type 2 diabetes and nonalcoholic hepatic steatosis when he was only 16 years old. [2]
2025: A study conducted in 9 European countries (including Italy) and published in Lancet positively associated consumption of ultra-processed foods with all-cause mortality as well as mortality from circulatory diseases, cerebrovascular disease, ischemic heart disease, digestive diseases, and Parkinson’s disease. A total of 428,728 participants (71.7 percent women) were included in the analysis, and 40,016 deaths were documented after a follow-up of more than 15 years. [3]
The issues of (un)proper nutrition and its impact on health, which are increasingly at the center of contemporary debate, are beginning to raise numerous questions about the possible responsibilities-even criminal ones-that can be found on the part of those who hold a position of guarantor with respect to individual food choices.
In particular, the issue becomes even more sensitive where children and adolescents suffer health damage, even in the long term. Parents and educators, on the one hand, and food companies, on the other, are increasingly held accountable for their respective choices and their consequences, including before the Courts.
With regard to the former, the judicial record, especially in the Anglosphere, is crowded with proceedings in which children and young people are removed from the care of their parents and placed in the care of social services because of the condition of obesity found by the courts. In some cases, as was the case with two little brothers in West Sussex (UK) [4], these were also children with good academic performance and excellent education, well integrated in their social context, whose parents, however, had repeatedly demonstrated an inability to manage their children’s diet, which combined intake of “junk food” and low physical activity: thus leading to unhealthy and worrying Body Mass Index values and to the orders of juvenile courts.
At the same time, public awareness and sensitivity to the nutritional components of commonly consumed foods is growing, and the political debate is intensifying-especially in Europe-about which food products should be taxed, discouraged or, conversely, protected. Within this framework, as mentioned and as will be discussed in more detail below, studies and research are increasing that identify a direct link between obesity (and several other diseases) and the consumption of “ultra-processed” foods.
Obesity is assuming epidemic characters worldwide, with alarming values particularly in the younger generation and trend projections that foresee a marked worsening of the phenomenon.
The World Obesity Federation estimates that by 2030, 50% of adults will have a high Body Mass Index (BMI). In fact, 33% of men and 28% of women will be overweight (BMI greater than 25 kg/m²), 12% and 14%, respectively, will be obese (BMI greater than 30 kg/m²), while 5% and 8% will be severely obese (BMI greater than 35 kg/m²) [5] and will have a high risk of developing other noncommunicable diseases that will require medical interventions. Childhood obesity is also growing steadily around the world: according to the 2025 report of the Lancet commission on adolescent health and wellbeing, 464 million young people will be overweight or affected by obesity by 2030, up from 143 million in 2015 [6].
Shifting the magnifying glass to our country, according to the latest data from the Istituto Superiore di Sanità, in 2023 19% of children were overweight and 9.8 were obese [7]. Regarding regional variability, higher prevalences are confirmed in the South and the Center than in Northern Italy, with marked differences between the top-ranked, autonomous province of Bolzano (overweight 12%, obese 3.3%) and the last, Campania (overweight 24.6%, obese 18.6%).
The consequences of obesity
Recent decades have also seen a significant increase in obesity rates in developing countries. This phenomenon may appear almost paradoxical, because we are talking about realities that have historically struggled with malnutrition and undernourishment, such as Mexico, India, China, or Thailand. This phenomenon is a concrete example of why obesity is currently considered a global epidemic. In fact, it would be a mistake to consider it as a disease of the individual, but, on the contrary, it is the result of numerous environmental and socio-economic factors, which strongly condition eating habits and lifestyles, leading to its spread with epidemic characteristics.
Economic development and income growth, at the same time, are directly proportional to the number of overweight and obese people. The factors that have led to this condition can be traced mainly to rapid urbanization: this has resulted, particularly for children, in sedentary lifestyles, accompanied by excessive use of electronic devices and television [8] and the gradual departure from normally recommended habits: healthy diet, sleep, physical activity. In addition to this have been the increased availability of ultra-processed foods, the rise of fast food and junk food (increasingly cheap and easily accessible) at the expense of fresh and nutritious foods (increasingly expensive)[9].
Widespread obesity in the population directly results in cardiovascular complications, such as hypertension, dyslipidemia, atherosclerosis, myocardial infarction, stroke, and increased likelihood of developing various types of cancers. Excess adiposity results among the main risk factors in developing metabolic diseases, including type 2 diabetes, as weight gain results in insulin resistance (insulin is the hormone that regulates blood sugar).
Again, obese patients often go on to experience respiratory and musculoskeletal diseases, nonalcoholic fatty liver, and, something not to be underestimated, psychological and psychiatric issues.
In addition to its direct health effects, obesity also has significant social and economic consequences: the condition is associated with increased work absenteeism, lower benefits, and high health care costs for treatment and long-term care.
The World Obesity Federation predicts that, if prevention and treatment measures are not improved, the global economic impact of overweight and obesity will reach $4.32 trillion annually by 2035. Equal to nearly 3 percent of global GDP, this impact is comparable to that of COVID-19 in 2020 [10].
These costs are directly related to the health care costs of treating obesity-related diseases, and indirectly, the cost is compounded by the loss of work productivity, disability, and premature mortality of obese individuals [11]. In addition, obesity is an important cause of long-term disability, and people with the condition have to live with discrimination and social prejudice on a daily basis [12].
Added to these are the biases that can also be found within courtrooms, where sometimes the weight of defendants and victims is used as a central argument in the assessment of facts. For both defendants and victims, their bodies may be perceived as beyond their control. According to this view, an overweight predator would be unable to restrain himself from committing crimes, just as a particularly corpulent victim would be unable to control his body to defend himself. Moreover, similarly to crime victims who belong to fragile groups, such as children, the elderly or those with mental illness, overweight victims may also be recipients of feelings of pity in courtrooms. However, in the opposite sense, in cases of abuse and violence, overweight women may not be taken seriously because of the stereotype that victims of these crimes are often imagined as thin people [13].
Childhood obesity
The onset of obesity in the early years of life has a worrisome impact on health, not only because these individuals will most likely remain obese as adults, but also because children/youth often present with metabolic, cardiovascular, respiratory, orthopedic complications, and nutritional deficits.
In essence, a clinical picture similar to that of an adult is found: according to a study conducted by Dr. Valerio Nobili, head of hepato-metabolic pathology at the Bambino Gesù, about 70 percent of overweight or obese children have nonalcoholic hepatic steatosis, an accumulation of fat in liver cells: these children have twice the risk of prediabetic condition and diabetes than healthy children [14].
Hypertension is also a complication that occurs in childhood: on average, the prevalence of this condition in children is 1-2% in normal weight, 5-6% in overweight, and 20-22% in obese [15].
What is more, the onset of obesity in adolescence, may result in alterations in puberty: in females, sexual maturation is anticipated; in fact, early telarche and menarche are observed [16], while in males it is delayed. Thus, the continuous increase in obesity in our society has resulted in spaced sexual maturation between the two sexes.
Hyperandrogenism (excess of androgens) is common in females, resulting in polycystic ovary syndrome, which is associated with altered menstrual cycle, acne, androgenetic alopecia, and marked insulin resistance [17].
In males, there is a high risk of low sperm motility [18], erectile dysfunction, low libido and reduced testosterone concentration, caused precisely by excess adipose[19]. All this results in reduced testicular volume and possible infertility in adulthood.
The causes of weight gain among adolescents
Three of the main causes of weight gain in adolescents we find incorrect eating habits in the first place. The study on food consumption in Italy, conducted by the CREA (Food and Nutrition Research Center), shows that Italian adolescents are below the intake levels recommended by the LARN (Reference Intake Levels of Nutrients and Energy for the Italian population), with regard to the consumption of vegetable proteins and foods that provide fiber: such as legumes, whole grains, fruits and vegetables. As for fruit, in particular, the average daily consumption among adolescents (146 g/day) and children (139 g/day) is much lower than in adults (194 g/day). As for vegetables, where the average consumption of the population is 147 g/day, it is only 86 g/day for children. In contrast, the tendency is to overconsume proteins and lipids of animal origin (cheese and meat, particularly red and processed meat) and high-glycemic-index carbohydrates, such as fruit juices, boxed breads, refined flours and industrial snacks[20].
According to ISS’s Health Behaviour in School-aged Children (HBSC) study, breakfast, considered the most important meal of the day, is eaten by only slightly more than half of young people between the ages of 11 and 17. There is also an excessive daily consumption of carbonated and/or sugary drinks (15 percent) and 1 in 4 adolescents consume sweets at least once a day. At the same time, there are low percentages of fruit and vegetable consumption (even below 30% in some age groups) consistent with the above data [21].
The ultra-processed foods
At this point, it is important to introduce the topic of the famous “ultra-processed foods,” around which the public debate of recent years has been raging.
In this regard, the most widely used classification is that of the NOVA system [ 22]], which subdivides foods according to the degree and purpose of industrial processing and includes 4 groups: unprocessed or minimally processed foods; foods processed in the kitchen for the purpose of extending shelf life; processed foods; and, indeed, ultra-processed foods.
Specifically, ultra-processed foods are formulations of ingredients, which are derived from a series of industrial processes (hence the term “ultra-processed”).
These processes include several steps: they may begin with the fractionation of whole foods (such as corn, wheat, soybeans, sugarcane, or beets) into substances that include only sugars, oils and fats, proteins, starches, and fibers; or with the shredding or grinding of animal carcasses, usually from intensive livestock farms. Some of these substances are then subjected to hydrolysis, hydrogenation or other chemical modification.
The next steps involve the assembly of these modified substances, with little, if any, whole foods present, using industrial techniques such as extrusion, molding and pre-frying. Dyes, flavorings, emulsifiers, and other additives are then frequently added to make the final product palatable or hyper-flavored. The processes end with sophisticated packaging, usually made of synthetic materials.
Sugar, oils, fats and salt are often major players in the ingredient list of these foods.
Sugar, in particular, is used in different forms, such as fructose, high-fructose corn syrup, fruit juice concentrate, invert sugar, maltodextrin, dextrose, and lactose. At the same time, the oils used are often modified (hydrogenated or interesterified oils).
As for additives, they include flavorings, flavor enhancers, coloring agents, emulsifiers, emulsifying salts, sweeteners, thickeners, and antifoaming, bulking, carbonating, foaming, gelling, and polishing agents. These mask unwanted sensory properties resulting from the ingredients, processes, and packaging used in the production of ultra-processed foods; they also impart sensory characteristics to the final product that are particularly attractive to see, taste, smell, and/or touch[23].
The processes and ingredients used in the production of ultra-processed foods are specifically designed to create highly profitable products: low-cost ingredients with long shelf lives, whether on supermarket shelves or in the home pantry. As a result, they tend to easily replace all other NOVA food groups.
Ultra-processed products, then, are not only the averse packaged snacks or carbonated drinks that we “indulge in once in a while,” but also a number of everyday consumer products that the average consumer would probably never include in this category. A particularly effective example of these products is yogurt.
As a result of highly effective marketing campaigns, contemporary fashion is geared toward “High Protein” products; thus, in this case, yogurts with added protein to make the product, already a protein source in itself, even more protein-packed.
Below are two photos corresponding to the labels and ingredient list of two types of yogurts: one defined as “protein” (photo 1 ) and one “normal” (photo 2).
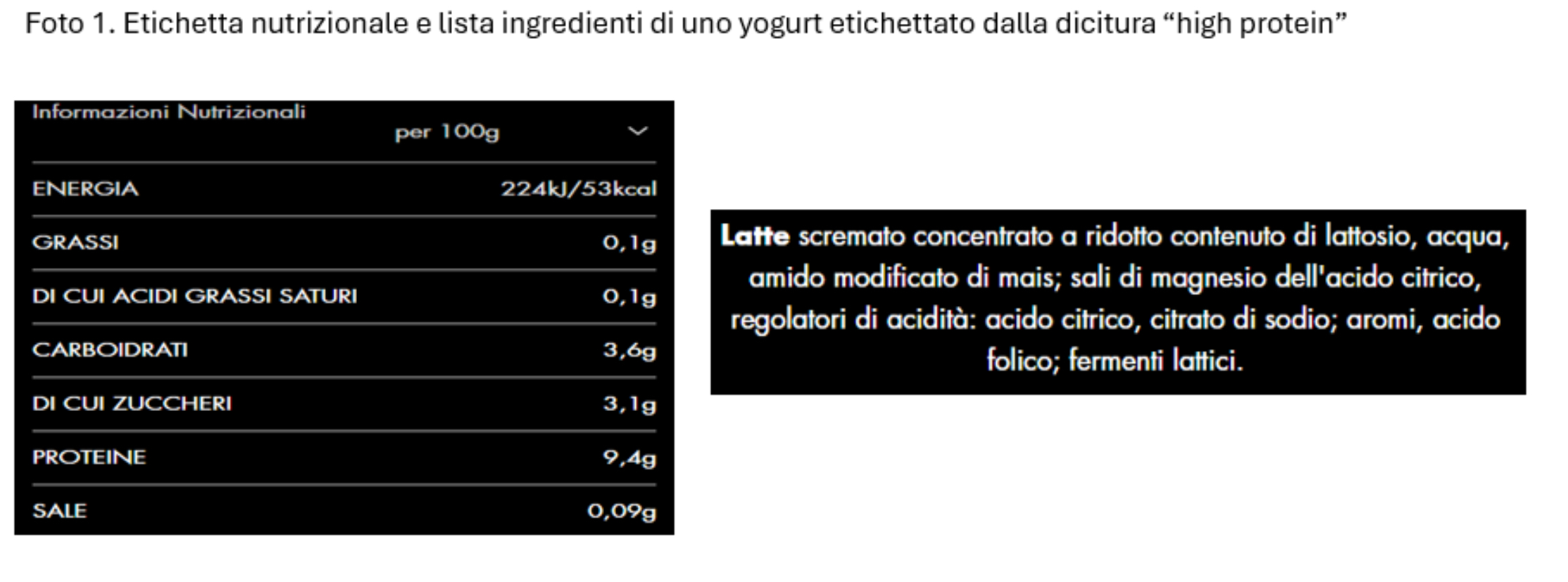
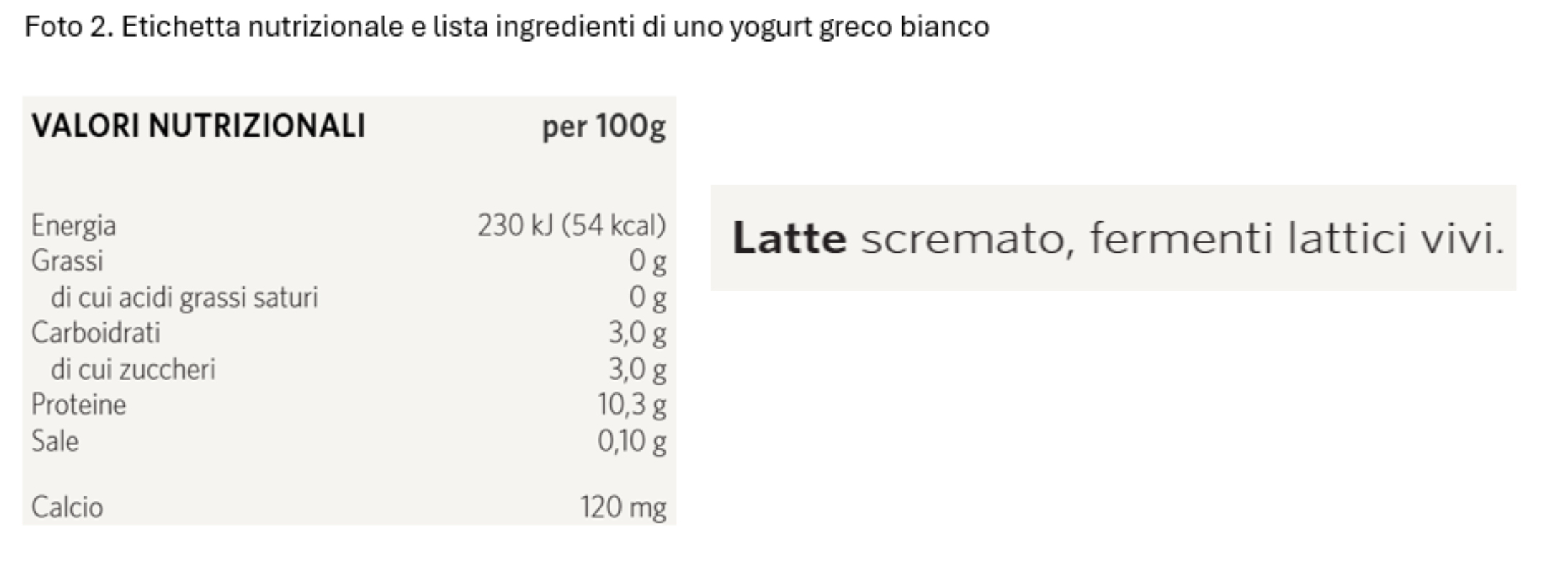 From reading the values, it is clear that, per 100gr of product, the one labeled as “high protein” has even less protein (9.4 g) than the “normal” one (10.3 g), with an ingredient list worthy of ultra-processed food classification.
From reading the values, it is clear that, per 100gr of product, the one labeled as “high protein” has even less protein (9.4 g) than the “normal” one (10.3 g), with an ingredient list worthy of ultra-processed food classification.
By comparing nutrition tables and ingredients from labels, as you just did for yogurt, you can see that many of the products that populate daily cupboards are highly processed.
Awareness and prevention
As analyzed above, obesity is a chronic multifactorial disease, and among the many reasons for its development, in recent years ultra-processed foods have emerged as a major determinant. Indeed, in a small volume of these products, hundreds of kcal are contained, yet they are not of good quality and do not provide useful nutrients to our bodies. On the contrary, the low fiber content and the prevalence of sugars, additives, and saturated fats make these foods precursors to several types of cancers, chief among them colorectal cancer[
[24]. Diets high in UPFs (ultra-processed foods), then, are related to an increased risk of diseases related to immune system dysregulation, such as inflammatory bowel disease (with alteration of the gut microbiota) and autoimmune diseases, such as multiple sclerosis and celiac disease[25]. Finally, some UPFs of animal origin and artificially sweetened beverages are particularly linked to an increased risk of developing type 2 diabetes[26].
In any case, it does not seem correct to “demonize” this food group and a priori oppose its consumption, which-if occasional-can be part of a healthy and balanced lifestyle without posing health risks.
What becomes more relevant is the overall diet of the individual, rather than the individual food, food group or single nutrient. The key word in this regard is awareness. Several factors contribute to the development of the latter. First, the marketing choices of large food companies assume an important role in the choices of consumers, who often tend to rely too easily on labels that extol seemingly beneficial features of products: no added sugar, high protein content, no palm oil, etc. The advancement of research and the consolidation of a widespread scientific basis for identifying harmful foods and production processes could force manufacturers to confront the growing risk of liability for injuries, including serious and permanent ones, caused by habitual consumption of products sold as harmless. Conversely, obligations to affix labels warning the purchaser of potential side effects could become more widespread: what is happening, for example, with alcohol products, tobacco derivatives or-increasingly-with unsaturated fats [27].
On the other hand, as far as children are concerned, the role – and responsibility – of parents is central, who will be asked to respond to a standard of care and dietary attention to which they are not yet accustomed – as shown also by Italian data on the nutrition of the youngest. In this regard, it will be essential first and foremost to raise awareness among adults so that they choose to adopt and teach children a healthy eating style from the earliest months of life. In this way, it will be possible to prevent the consolidation of wrong and potentially harmful eating habits in later years.
As noted in one of the court orders above[28], being present and loving parents, in the context of a happy family, is no longer sufficient to meet the health needs of children, especially where the severity of problems resulting from overweight or obesity are not fully understood.
Dr. Maddalena Cotardo, Biologist Nutritionist
Antonio Laudisa, Criminal Attorney
References
[1] https://www.judiciary.uk/wp-content/uploads/2023/03/R-v-Lloyd-Jones-Titford-sentencing-010323.pdf
[2] https://www.forthepeople.com/sites/default/files/2024-12/Filed%20UPF%20Complaint.pdf
[3] González-Gil, Esther M. et al, Associations between degree of food processing and all-cause and cause-specific mortality: a multicenter prospective cohort analysis in 9 European countries
[4] https://www.bailii.org/ew/cases/EWFC/OJ/2020/B62.html
[5] World Obesity Atlas 2025, World Obesity, March 2025, https://s3-eu-west-1.amazonaws.com/wof-files/World_Obesity_Atlas_2025_rev1.pdf
[6] Amouzou, A., Barros, A.J.D., Requejo, J., Faye, C., Akseer, N., Bendavid, E., Blumenberg, C., Borghi, J. , El Baz, S., Federspiel, F., Ferreira, L.Z., Hazel, E., Heft-Neal, S., Hellwig, F., Liu, L., Maïga, A., Munos, M., Pitt, C., Shawar, Y.R., Shiffman, J., et al. (2025). The 2025 report of the Lancet Countdown to 2030 for women’s, children’s, and adolescents’ health: tracking progress on health and nutrition. The Lancet 405 (10488) 1505-1554. 10.1016/S0140-6736(25)00151-5.
[7] https://www.epicentro.iss.it/okkioallasalute/pdf2024/INFOGRAFICA%20OKKIO%202023_2%20maggio%20DEFINITIVA.pdf
[8] Florida Atlantic University. “Alarming surge: Global crisis of childhood overweight and obesity.” ScienceDaily. ScienceDaily, September 26, 2024. www.sciencedaily.com/releases/2024/09/240926131942.htm.
[9] Monteiro, C.A., Moubarac, J.-.-C., Cannon, G., Ng, S.W. and Popkin, B. (2013), Ultra-processed products: global dominance. Obes Rev, 14: 21-28 . https://doi.org/10.1111/obr.12107.
[10] World Obesity, Economic impact of overweight and obesity to surpass $4 trillion by 2035, March 2, 2023, https://www.worldobesity.org/news/economic-impact-of-overweight-and-obesity-to-surpass-4-trillion-by-2035
[11] Bramming M, Jørgensen MB, Christensen AI, Lau CJ, Egan KK, Tolstrup JS. BMI and Labor Market Participation: A Cohort Study of Transitions Between Work, Unemployment, and Sickness Absence. Obesity (Silver Spring). 2019 Oct;27(10):1703-1710. doi: 10.1002/oby.22578. PMID: 31544342.
[12] Nutter S, Russell-Mayhew S, Alberga AS, Arthur N, Kassan A, Lund DE, Sesma-Vazquez M, Williams E. Positioning of Weight Bias: Moving toward Social Justice. J Obes. 2016;2016:3753650. doi: 10.1155/2016/3753650. Epub 2016 Sep 22. PMID: 27747099; PMCID: PMC5055973.
[13] Elizabeth Beety, Valena (2013) “Criminality and Corpulence: Weight Bias in the Courtroom,” Seattle Journal for Social Justice: Vol. 11: Iss. 2, Article 4, https://digitalcommons.law.seattleu.edu/sjsj/vol11/iss2/4; Tracy Royce, The Shape of Abuse: Fat Oppression as a Form of Violence Against Women, in THE FAT STUDIES READER 151, 153 (Esther Rothblum & Sondra Solovay eds., 2009), https://dokumen.pub/the-fat-studies-reader-9780814777435.html.
[14] Children and diabetes: double the risk if the liver is fatty – Bambino Gesù Children’s Hospital, https://www.ospedalebambinogesu.it/bambini-e-diabete-rischio-doppio-se-il-fegato-e-grasso-90316/
[15] Simonetta Genovesi, Laura Antolini, Marco Giussani, et al. Hypertension, Prehypertension, and Transient Elevated Blood Pressure in Children: Association With Weight Excess and Waist Circumference, American Journal of Hypertension, Volume 23, Issue 7, July 2010, Pages 756-761, https://doi.org/10.1038/ajh.2010.50.
[16] Itriyeva K. The effects of obesity on the menstrual cycle. Curr Probl Pediatr Adolesc Health Care. 2022 Aug;52(8):101241. doi: 10.1016/j.cppeds.2022.101241. Epub 2022 Jul 21. PMID: 35871162; PMCID: PMC9449629.
[17] Ibid.
[18] Leisegang K, Sengupta P, Agarwal A, Henkel R. Obesity and male infertility: Mechanisms and management. Andrology. 2021 Feb;53(1):e13617. doi: 10.1111/and.13617. Epub 2020 May 12. PMID: 32399992.
[19] vKhodamoradi, Kajala; Parmar, Madhumitaa; Khosravizadeh, Zahrab; Kuchakulla, Manisha; Manoharan, Meenakkshyc; Arora, Himanshua,d. The role of leptin and obesity on male infertility. Current Opinion in Urology 30(3):p 334-339, May 2020. | DOI: 10.1097/MOU.0000000000000762.
[20] https://www.crea.gov.it/web/alimenti-e-nutrizione/-/iv-scai-studio-sui-consumi-alimentari-in-italia
[21] https://www.epicentro.iss.it/hbsc/pdf/temi2022/abitudini-alimentari-2022.pdf
[22] FAO, Ultra-processed foods, diet quality, and health using the NOVA classification system, https://www.fao.org/fsnforum/resources/trainings-tools-and-databases/ultra-processed-foods-diet-quality-and-health-using-nova
[23] Monteiro CA, Cannon G, Levy RB, Moubarac JC, Louzada ML, Rauber F, Khandpur N, Cediel G, Neri D, Martinez-Steele E, Baraldi LG, Jaime PC. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. 2019 Apr;22(5):936-941. doi: 10.1017/S1368980018003762. Epub 2019 Feb 12. PMID: 30744710; PMCID: PMC10260459.
[24]
Association of ultra-processed food consumption with colorectal cancer risk among men and women: results from three prospective US cohort studies, British Medical Journal, 2022
[25] Maki, K.A., Sack, M.N. & Hall, K.D. Ultra-processed foods: increasing the risk of inflammation and immune dysregulation? Nat Rev Immunol 24, 453-454 (2024). https://doi.org/10.1038/s41577-024-01049-x.
[26] Food consumption by degree of food processing and risk of type 2 diabetes mellitus: a prospective cohort analysis of the European Prospective Investigation into Cancer and Nutrition (EPIC), Dicken, Samuel J. et al, The Lancet Regional Health – Europe, Volume 46, 101043.
[27] https://www.who.int/news/item/07-12-2021-countries-with-regulations-protecting-people-from-industrially-produced-trans-fat-tripled-over-the-past-year
[28] https://www.bailii.org/ew/cases/EWFC/OJ/2020/B62.html
